We are far enough into this pandemic that there really is no excuse that folks still don’t know about the importance of going into quarantine after being exposed or why you should practice social distancing and wear a face mask.

And yet, cases are once again surging all over the country…
7 Things to Know About COVID-19
In addition to knowing that the pandemic isn’t over and won’t be over for some time, you should know that:
- you could have been exposed to SARS-CoV-2 if you had close contact (less than 6 feet apart) to someone with COVID-19 (has symptoms or tested positive) for at least 15 minutes, even if you were both wearing masks (sure, there is much less risk if you were wearing masks, but to be safe, it still counts as an exposure). And with the latest guidelines, the exposure doesn’t have to for a continual 15 minutes, but rather “a cumulative total of 15 minutes or more over a 24-hour period.” So if you were close to someone with COVID-19 for 5 minutes each hour for three hours, then that counts as close contact. Fortunately, if you are fully vaccinated, including a booster dose, this kind of close contact does not mean that you have to go into quarantine, unless you develop symptoms of COVID.
- you can develop symptoms of COVID-19 from one to 14 days after you are exposed to someone with COVID-19. This is the incubation period for the SARS-CoV-2 virus and the time you should be in quarantine after your exposure (although there are some new options to end quarantine early).
- testing negative soon after you are exposed to someone with COVID-19 doesn’t mean that you can’t develop symptoms later in your incubation period! Although testing is a very important part of containing this pandemic, you don’t necessarily need to rush to get tested right after you are exposed. You can, but understand that an early negative test doesn’t get you out of your quarantine. A positive test will shift you into a period of isolation, but know that some COVID-19 tests, especially the rapid antigen tests, are more likely to give a false positive result if you don’t have symptoms. If you are going to get tested after being exposed and don’t have symptoms, the optimal time is probably about 5 to 7 days after your exposure and remember to continue your quarantine if it is negative, or at the very least, wear a mask (part of the guidelines to end quarantine early).
- you can be contagious for at least two days before you develop any symptoms of COVID-19 or test positive and will continue to be contagious for at least ten days, the time you should be in isolation (a stricter form of quarantine). If you had severe symptoms or have a severely weakened immune system, then you might be contagious for a much longer period of time though, up to 20 days. And remember that you can continue to test positive for weeks or months, long after you are no longer contagious, which is why repeat testing is no longer routinely recommended. As with quarantine, there are options to end isolation early, after 5 days if your symptoms are getting better (or no symptoms), as long as you wear a mask for another 5 days.
- you can be contagious even though you don’t have symptoms, which is why, if you are unvaccinated or high risk, you should try to always wear a mask and practice social distancing when you are around other people. You don’t know who has COVID-19!
- if you continue to be exposed to someone with COVID-19 in your home, your 14 day quarantine period doesn’t start until they are no longer contagious, as you will continue to be exposed that whole time. That’s why some folks end up in extended quarantine for 24 days- the 10 days that the COVID-19 positive person was contagious + 14 days of quarantine, which started once the person was no longer contagious. You may be able to shorten this period with the new guidelines though.
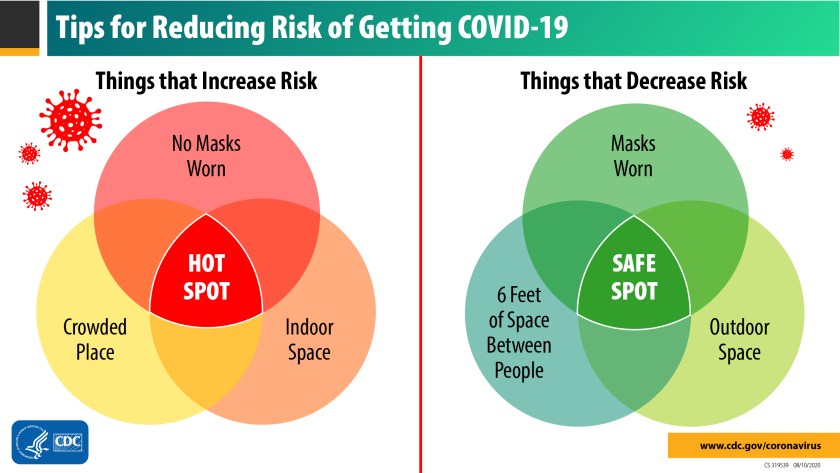
- we can’t count on natural herd immunity to end the pandemic, as that would mean millions and millions of people dying. But understand that there is a middle ground between the extremes of total lockdowns and doing nothing. Wear a mask, keep six feet apart from other people (social distancing),and avoid crowds until you can get vaccinated and protected!
Most importantly, know that the more people you are around, the higher the risk that you will be exposed to and get sick with COVID-19.
Is it really essential that you have a family gathering with 25 or 50 people right now, as cases once again begin to surge in your area because of the Delta Omicron variant? Will you be able to keep everyone six feet apart? Will they be wearing masks the whole time?
Do you want to keep schools and businesses open?
Then get vaccinated and protected!
And if you can’t get a vaccine, wear a mask, practice social distancing, wash your hands, avoid crowds, and stop acting like the pandemic is already over or never existed in the first place!
More on COVID-19
- COVID-19 Vaccination Questions and Answers
- Get All of Your COVID-19 Questions Answered
- What to Do if You Have Been Exposed to COVID-19
- What to Do if You Have Been Diagnosed with COVID-19
- Returning to Sports After Having COVID-19
- Why Are Social Distancing Kids Still Getting Sick?
- Are Kids Dying With COVID-19?
- Who Are the Real COVID-19 Experts?
- Why There is Still So Much COVID-19 Confusion
- CDC – Public Health Guidance for Community-Related Exposure
- CDC – Interim Public Health Recommendations for Fully Vaccinated People
- CDC – When to start and end quarantine
- CDC – Isolate If You Are Sick
- CDC – Discontinuation of Isolation for Persons with COVID-19 Not in Healthcare Settings
- CDC – When You Can be Around Others After You Had or Likely Had COVID-19
- COVID-19 Risks for Various Activities
- CDC – Deciding to Go Out
- CDC – Clinical Questions about COVID-19: Questions and Answers
- Johns Hopkins Coronavirus Questions and Answers
- WHO – Q&A on coronaviruses (COVID-19)
- ECDC – Q & A on COVID-19
- FDA – Coronavirus Disease 2019 (COVID-19) Frequently Asked Questions
- COVID-19 Diagnostic Testing Redux
- Top COVID-19 Questions, Answered: An Interview with ASM President Robin Patel
- 31 questions and answers about COVID-19 (Bill Gates)
- COVID-19: Frequently asked questions (AMA)
- Transmission dynamics reveal the impracticality of COVID-19 herd immunity strategies
- Scientific consensus on the COVID-19 pandemic: we need to act now
- expert reaction to Barrington Declaration, an open letter arguing against lockdown policies and for ‘Focused Protection’
- ‘It’s been so, so surreal.’ Critics of Sweden’s lax pandemic policies face fierce backlash
- Focused Protection, Herd Immunity, and Other Deadly Delusions


























You must be logged in to post a comment.